Abbreviations:
- PP = Planned Parenthood
- CHC = Community Health Center
- RHC = Rural Health Clinic
List of Questions
- What exactly is – a Community Health Center? A Rural Health Clinic? A County Health Center? A Campus Health Center? Telehealth?
- Why are Crisis Pregnancy Centers or Pregnancy Help Centers usually not listed?
- Do you need to mention this is a PP-alternatives campaign when it’s not helpful?
- What about Catholics or others who don’t want to have anything to do with artificial contraception?
- What about Health Centers that are pro-PP?
- What if the proposed alternative center offers possibly abortifacient drugs and/or refers for abortions?
- Why focus on trivial points, rather than making a full case for being pro-life?
- What about taxpayer defunding or foundation defunding?
- What kinds of facilities does PP have? This question has now been moved to its own page.
- How do we show that we need alternatives to Planned Parenthood? This question is now answered on the page Donors to Planned Parenthood.
1. What exactly is:
A Community Health Center?
Federally-qualified Community Health Centers go through an application process to fit all the regulations needed to be a CHC. Other health centers may be suitable as PP alternatives, but they haven’t applied.
CHCs are supposed to operate under the direction of patient-majority governing boards, offer services regardless of ability to pay, be sensitive to local needs, and offer primary care plus supportive services. There are thousands of CHCs throughout the country, especially in large cities, where it’s common to have several locations in the same local chain. They’re common in rural locations and small towns as well, but are less prevalent there.
By definition, they don’t do abortions. They vary in what the staff’s attitude toward abortion is.
We got our information from the federal Find a Health Center website in which the PP address can be put in and a list of locations within 5 miles will be generated (or further if there are none within 5 miles).
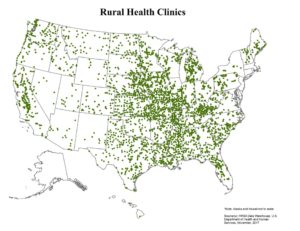
A Rural Health Clinic?
Rural Health Clinics are offered under a different federal program, intended to increase services for Medicaid and Medicare patients in rural areas. States vary widely in how many they have –New York State had only nine, whereas Missouri had over 300. In July of 2018, the total number in the United States was 4,277. Unlike CHCs, they’re not obligated to offer service to uninsured or low-income people, so this feature would need to be checked in individual cases. While CHCs must be nonprofit or public, the RHCs can be either nonprofit or for-profit. They’re expected to be in under-served and non-urban areas.
We got our information on locations from a lengthy pdf document at www.cms.gov; however, as of March, 2019, the document is no longer on the web. We’ll check again occasionally, but our listings are based on the old document that can no longer be referred to. Local web searches may be able to find more information.
A County Health Clinic?
These are clinics run by county governments, and vary widely in the amount and quality of their services and whether or not they’re overcrowded. We generally check into them only for locations that don’t have CHCs or RHCs, but local people may be aware that their own county clinics have a good reputation and may want to consider them.
A Campus Health Center?
These vary widely in what they offer and generally only serve students. That makes them quite limited as PP alternatives. Yet they’re important to consider, since college students are one of PP’s main target audiences, and especially vulnerable to abortion pressures.
A Teaching Hospital?
Sometimes hospitals or clinics associated with medical schools offer services to low-income people to help in training new doctors and other medical personnel. Unlike CHCs and RHCs, these might do abortions, so we usually put a caution note when we list them. If we find out they do abortions, we’ll put that as a warning on the list.
Those that only serve children, veterans, or specialize in something like cancer care weren’t included. When local activists or a perusal of their websites tell us they don’t really offer the services needed or are otherwise unsuitable, we don’t list them.
For the most part, we add these in order to have extra options when the options are low. When there are an ample number of other alternatives, we either skip it, or link back to the list of teaching hospitals in the event local activists find that useful – say, if all the CHCs are problematic, or if the teaching hospital is known to be especially good in some way.
Telehealth?
Modern technology allows for some forms of medicine to be practiced on the web. Telehealth has been growing for some time, but then got a huge boost from the Covid-19 crisis. PP has now vastly expanded its practice, and so we have a full page on Telehealth.
2. Why are Crisis Pregnancy Centers or Pregnancy Help Centers usually not listed?
They offer alternatives to abortion, but generally don’t provide the actual medical services that PP does, especially for women who aren’t pregnant, and for men who use PP for such things as STD testing. We do include medical clinics designed by pro-lifers, such as Obria, Guiding Star, and Marisol; see Pro Women’s Health Care Centers, a consortium of autonomous centers.
We’ll include other centers if they provide the services PP does, beyond pregnancy tests and ultrasounds, such as STD screenings and treatment, Urinary Tract Infection (UTI) treatment, or cancer screenings. We encourage pregnancy help centers, especially those already deliberately near PP centers, to consider adding those services if they can.
Nevertheless, there will be women and men – especially clients who use PP – who will disdain going to a place that’s clearly pro-life. Therefore, knowledge of other health centers as we have listed could still be crucial for convincing people to going elsewhere.
3. Do you need to mention this is a PP-alternatives campaign when it’s not helpful?
Under no circumstances should this be lied about, of course. If you’re asked point-blank, then you’re upfront about it. Yet if honesty doesn’t require you to bring it up, as when you’re working in coalitions, it isn’t necessary.
For example, say that you’re on a campus where the health center offers STD screening only if patients have symptoms but not for general screening. Your group decides on a campaign to get the health center to expand its services. The fact that this will draw business away from PP is one of your motivations. Yet it’s a good cause in itself, and you can probably get other groups on campus to join in the campaign just on its own merits. There should be no deception about your own motivation, but this doesn’t need to be highlighted.
As another example, say that a consortium of health advocacy groups is trying to get the state legislature to fund the establishment of more medical clinics for low-income people. You have in mind some specific spots near PP centers that are currently under-served, but the bill includes far more than those. You support the entire bill, both because of the centers near PPs, and also because the entire bill is a good idea. Again, there should be no deception, but it’s not necessary to highlight a specific motivation.
Coalitions often involve people who disagree on various other issues still getting together to focus on one, and joining coalitions will often be the most effective strategy.
4. What about Catholics or others who don’t want to have anything to do with artificial contraception?
Most of the alternative medical facilities we list provide artificial contraception. Many people who don’t want to feel any responsibility for promoting this practice might still feel comfortable moving people from PP to another center, since no greater use of artificial or hormonal contraception has occurred than would have otherwise. Getting people away from PP is so important.
However, some people aren’t comfortable with any sense of participation in any way. We encourage people to take actions they’re most comfortable with and most enthusiastic about. Some possibilities for those who don’t want to simply refer people from PP to another place that provides artificial contraception:

Any alternative way of providing low-cost, private and confidential STD testing and treatment can make a huge difference. This is so important that we a have a full page covering information on STD testing.
PP has also recently highlighted services for treating Urinary Tract Infections (UTI). See our page on Telehealth for more information about UTI treatment. Letting people know of alternative ways to get this treatment is easy, and another way to pull away from PP’s influence.
Find out the best places for cancer screening (breast exams and pap smears) and for STD testing and treatment. If you find some you’re comfortable with, do the homework to explain why they’re better than PP. Then you can make a pitch to people who now refer to PP to see if they can be talked into referring elsewhere. Remember, a lot of times the only reason they refer to PP is that it has better name recognition, or PP may have assertively sought the referrals. If you handle it well, those referring may be grateful for the information.
You can also use other venues to publicize the availability of the screening services mentioned above – for example, colleges, people leaving concerts, or churches that are currently using PP materials.
Several of the PP centers have health violation documents, malpractice suits, ambulance calls and other problems. That can be useful as a way to persuade places that include PP in lists of resources to take that that center off the list. The website Problems at Planned Parenthood keeps a constantly updated list of documentation of these for each center.
Nearby Pregnancy Help Centers can be encouraged to add STD testing and treatment, UTI treatment, and/or cancer screenings. If that’s workable, they may need a lot of fundraising and other practical help to do it.
The really ambitious can support establishing mobile clinics with suitable services near the PP centers.
5. What about Health Centers that are pro-PP?
While CHCs by definition don’t perform abortions themselves, the alternative centers we’re looking at will probably vary widely in their attitudes towards PP. Some will have pro-lifers on staff, and others may have staff members who show up to pro-PP rallies.
Most websites of CHCs don’t mention PP one way or the other, but we do occasionally find on their websites that they mention some connection. In the case of an intense  cooperative arrangement, such as doctors getting training in “reproductive health,” then perhaps finding a better place for such training would be a worthwhile tactic. We flag places with a substantial link with this “PP Connection Caution” graphic.
cooperative arrangement, such as doctors getting training in “reproductive health,” then perhaps finding a better place for such training would be a worthwhile tactic. We flag places with a substantial link with this “PP Connection Caution” graphic.
Yet the main way of finding out their attitude to PP will be on the visits, rather than the web page. Do they have PP brochures on their literature racks? Do they refer to PP?
Any pro-PP sentiment will be difficult to stomach, but the next question is: Are we still better off if women go to the CHC (or other clinic), rather than have a habit of going to PP? If a women who isn’t pregnant is accustomed to getting regular gynecological and cancer screening care at PP, then that’s where she may well go when she gets pregnant, and there she’ll face an assumption that she wishes to “terminate.” At the CHC, even if they would refer her for an abortion if she asked, she may have to ask. There will be CHCs where the first assumption when the pregnancy test comes back positive is that she goes to the prenatal clinic, which many have right there. This could be life-saving.
Note also that many CHCs are in chains sharing the same web page, and individual centers within a chain may have different attitudes on this topic.
6. What if the proposed alternative center offers possibly abortifacient drugs and/or refers for abortions?
Some people will lose all enthusiasm under these circumstances, if these nearby health centers are the only options. But consider: Taking business away from PP is a positive thing. Money PP doesn’t get can’t be channeled into abortion activism, lobbying, and pushing abortion on others. Any money adds to their legislative arm and political activities. Money is fungible – any money coming into PP promotes abortion even if that money doesn’t directly pay for abortions. The less money they have, the less they can do.
7. Why focus on trivial points, rather than making a full case for being pro-life?
Given the repulsiveness of feticide and our passion for ending it, do we really care if we get three people to go to a CHC for an STD test because we’ve told them it would save them $10? Shouldn’t we be spending our time explicitly educating about how wrong abortion is so that people won’t patronize PP?
One method of changing people’s minds about any form of violence is to lay out the full case of what’s wrong and hope to persuade them. This is crucial work, but if it were enough, the issue would have been settled long ago.
Another method of changing people’s minds is to change their behavior. People have a drive to have their thoughts and behavior match, and if they don’t, it causes them stress (in psychology, this is called “cognitive dissonance”).
Therefore, when people change their behavior, they’re way more likely to be persuaded of the entire case. Their mental drive for consistency between attitudes and actions can change their attitudes.
A historical example of a kind of violence that seemed so very intractable is legally-enforced racial segregation. With the Montgomery bus boycott to end segregation on the buses in Montgomery, Alabama, business leaders eventually found it in their best business interests to allow for the racial integration being demanded. Years later, surveys showed that their racial attitudes had changed for the better, more in line with racial equality. A cynic could say this was due to greed rather than a change of heart. Greed may have been what changed the behavior, when it over-rode the racial prejudice. Once the behavior changed, however, so did the racial prejudice. When people noticed they were behaving in a new way, they accounted for their behavior by adopting an attitude that was consistent with the behavior.
This can happen here, too. Anything that causes a person to go somewhere else, rather than PP, will help change attitudes in the long run. It doesn’t matter how trivial or uninspiring the reason is. The behavior change is worthwhile not only because it directs money away from PP. Changed behavior is also one of the best ways of getting to changed attitudes – and that makes all the changes more permanent.
8. What about taxpayer defunding or foundation defunding?
Impact on lobbying (37 seconds)
Efforts to persuade legislators to cut the funding will be more effective if we can disprove PP’s argument that they’re needed in under-served areas – either because we can document that these areas are well-served, or because we found that they were indeed under-served (at least for those of low income) but we’ve worked to see to it that women and men now have better health care options than PP. Such efforts will also be more effective when the number of people going elsewhere is greater and the number going to PP is fewer, making it possible to argue that the governmental resources should be going to where the people are going.
Federal taxpayer defunding through the presidential administration can vary with the administration, but it will cover only Title X family planning grants. The Medicaid payments in most states will still go to PP as long as women decide to go to PP. While there are states that are cutting PP off Medicaid (and the US Supreme Court is hearing arguments about whether to let them do so on April 2, 2025), there will certainly be many states that won’t, so getting Medicaid patients to go elsewhere will be the only taxpayer defunding method in those states.
As for foundations, the pro-life movement has been successful in getting many foundations to withdraw their funding for PP. But this will become all the easier to do when the number of clients going to PP goes down. PP will seem like a less worthy expenditure of foundations’ dollars if its client base is smaller.
Individuals feel more encouraged to make donations to PP when there’s a local PP center that provides tangible indications of what they do. Local centers are also useful bases for PP to recruit volunteers. When centers close, or seem not to be doing so much, it might decrease individual donations and volunteering.
We need to build up nonviolent institutions to replace violent institutions. This happens when PP funding is not merely cut, but goes elsewhere – into filling the real medical needs of vulnerable people.
For more on directly trying to persuade individuals, groups, and foundations not to donate, see our page Donors to Planned Parenthood.
Other questions?
Feedback is much appreciated. This is the kind of project where new ideas, new information, and new stories to share pop up all the time. We update this site frequently. Please send any thoughts or information to grassrootsdefunding@consistent-life.org.
We also encourage you to send in success stories, or why something that looked like a good idea turned out to be a mistake, or anything else good to share with other activists. Those will go in our blog.